






You hear the visiting nurse say “raise him to Semi-Fowler’s” and freeze. She might as well have spoken Latin. But these hospital bed position names aren’t medical jargon reserved for clinicians — they describe specific angles that directly affect breathing, digestion, circulation, and skin health. If you’re caring for someone at home, knowing what each position does (and when to use it) can make the difference between a comfortable night and a 3 a. m. crisis.
This guide breaks down every standard hospital bed position by name, angle, and purpose — so the next time a healthcare provider gives you positioning instructions, you’ll know exactly what to do.
Why Hospital Bed Position Names Matter for Home Caregivers
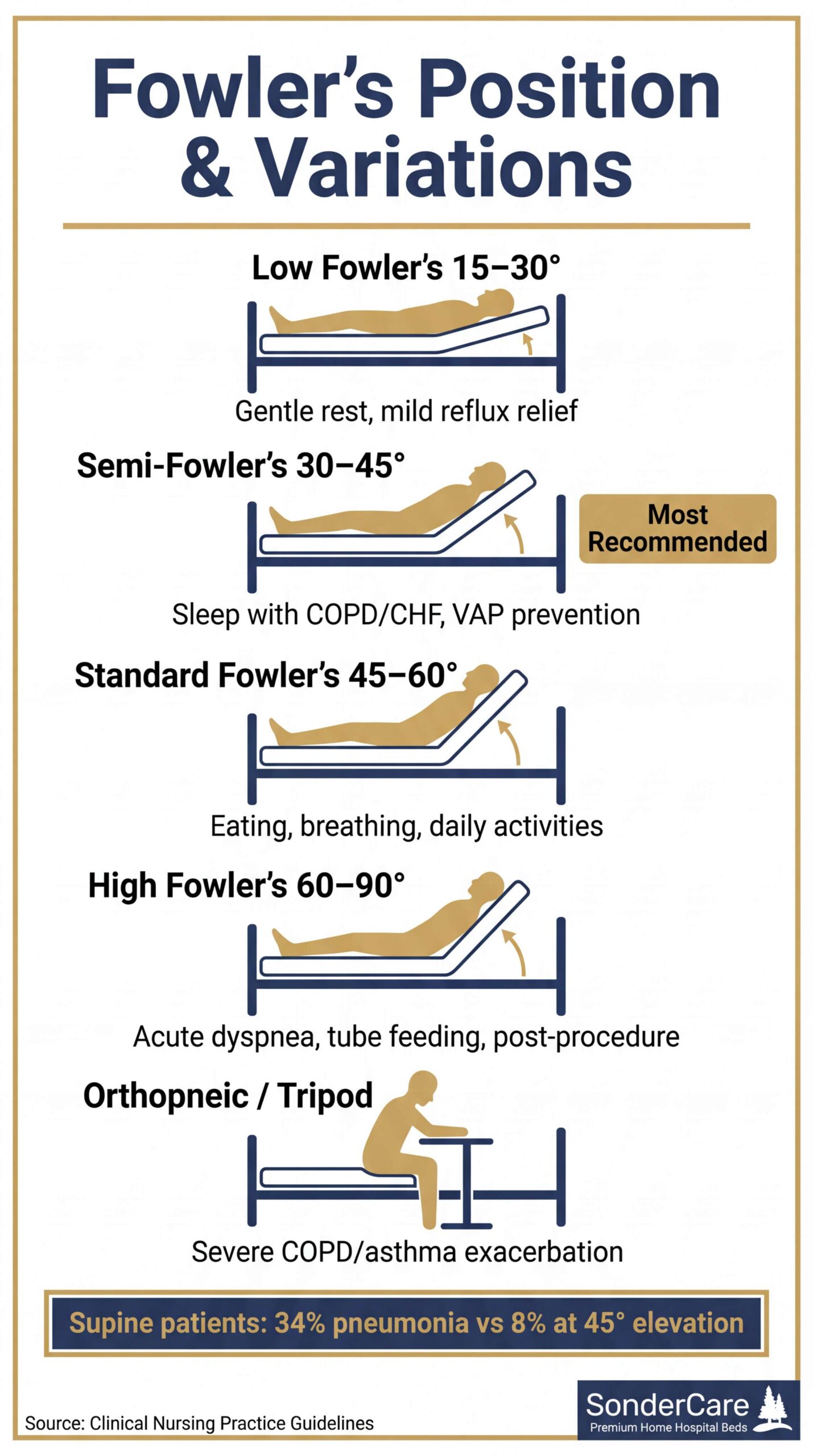
Clinical positioning isn’t just hospital protocol. Research shows that something as simple as head-of-bed angle can significantly impact patient outcomes. In one landmark study, patients kept flat (supine) developed pneumonia at a rate of 34%, compared to just 8% among those elevated to 45 degrees1. That’s a fourfold difference from a single positioning change.
For home caregivers managing conditions like COPD, heart failure, acid reflux, or post-surgical recovery, understanding these positions means you can follow medical instructions precisely — and adjust between doctor visits when your loved one’s comfort changes.
Modern home hospital beds like the SonderCare Aura Premium replicate nearly every clinical position through programmable presets, giving caregivers push-button access to Fowler’s, Trendelenburg, and everything in between.
Fowler’s Position and Its Variations
Fowler’s position is the one you’ll use most. Named after surgeon George Fowler, it simply means the head of the bed is elevated while the patient remains on their back. The variations differ only by angle — but those degrees matter.
Standard Fowler’s Position (45-60 Degrees)
The head of the bed is raised to 45-60 degrees, creating a semi-sitting posture. This is the go-to position for:
- Eating and drinking — Reduces aspiration risk. A videofluoroscopic study found that a 45-degree reclined posture significantly reduced penetration-aspiration scores in patients with swallowing difficulties2
- Breathing comfort — Opens the airway and allows the diaphragm to drop, increasing lung capacity
- Reading, watching TV, or visiting — The most natural “awake” position for daily activities
High Fowler’s Position (60-90 Degrees)
Nearly upright, like sitting in a straight-backed chair. Used when maximum lung expansion is needed — during acute breathing difficulty, post-thoracic procedures, or when a patient needs to sit fully upright for tube feeding. This position requires a bed with reliable back-angle adjustment to hold the steep incline safely.
Orthopneic Position (The “Tripod”)
Sometimes High Fowler’s isn’t enough. During a COPD exacerbation or severe asthma attack, the patient may need to sit fully upright and lean forward, resting their arms and head on an overbed table cushioned with pillows. This is the orthopneic or “tripod” position.
Leaning forward lets the diaphragm drop completely and recruits the accessory muscles in the chest and shoulders to pull air in. If your loved one has severe respiratory episodes at home, this is the position to know. You’ll need the bed raised to High Fowler’s, an overbed table positioned across the bed, and two or three pillows stacked on top for the patient to lean into.
Semi-Fowler’s Position (30-45 Degrees)
The most clinically recommended “resting” elevation. A 2022 multi-society guideline from the CDC, SHEA, and IDSA classifies keeping the head of bed at 30-45 degrees as an essential practice for preventing ventilator-associated pneumonia3. For home care, Semi-Fowler’s is the default sleeping position for patients with:
- COPD or chronic breathing difficulty — Keeps airways open without the fatigue of sitting fully upright
- Congestive heart failure — Reduces fluid pooling in the lungs
- Acid reflux (GERD) — Gravity keeps stomach acid from traveling up the esophagus
Low Fowler’s Position (15-30 Degrees)
A gentle incline, barely noticeable. Used for patients who need slight elevation for comfort or drainage but find higher angles uncomfortable. Often used during sleep for patients recovering from certain surgeries.
Quick Reference: Fowler’s Variations
| Position | Angle | Primary Use |
|---|---|---|
| Low Fowler’s | 15-30 degrees | Gentle rest, mild reflux relief |
| Semi-Fowler’s | 30-45 degrees | Sleep with COPD, CHF, VAP prevention |
| Standard Fowler’s | 45-60 degrees | Eating, breathing, daily activities |
| High Fowler’s | 60-90 degrees | Acute dyspnea, tube feeding, post-procedure |
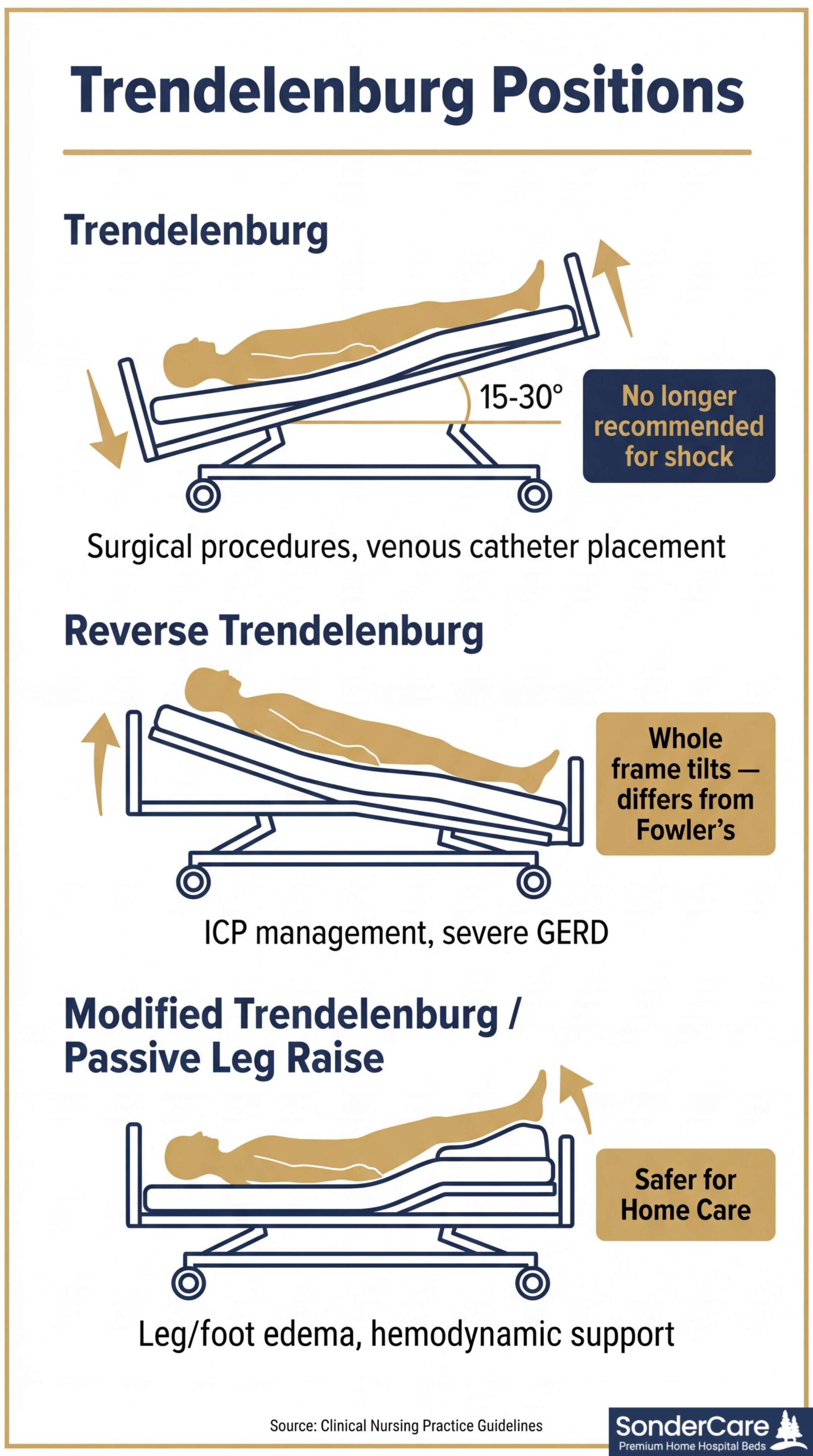
Trendelenburg Position
In Trendelenburg position, the entire bed tilts so the patient’s head is lower than their feet, typically at 15-30 degrees. This position carries the name of German surgeon Friedrich Trendelenburg, who used it during pelvic surgery.
Clinical uses include:
– Certain surgical procedures requiring lower abdominal access
– Central venous catheter placement (improves venous filling)
– Specific neurological assessments
A 2024 meta-analysis of 16 studies found the position increases stroke volume by approximately 11%, which is why it was historically used in shock treatment4. However, contemporary guidelines no longer recommend routine Trendelenburg for shock because it increases intracranial pressure and can compromise breathing.
Home care note: Most caregivers will rarely use Trendelenburg at home. But if a physician prescribes it for specific situations, you’ll need a bed that tilts the entire frame — not just the head section. The SonderCare Aura Platinum offers full Trendelenburg capability through its motorized frame tilt, a feature missing from most consumer adjustable beds.
Reverse Trendelenburg Position
The opposite of Trendelenburg: the head is elevated above the feet by tilting the entire bed frame. This is different from Fowler’s, where only the back section bends upward — in Reverse Trendelenburg, the patient stays flat while the whole frame angles.
This distinction matters clinically. Research on craniotomy patients found that a 10-degree Reverse Trendelenburg tilt reduced intracranial pressure from 9.5 to 6.0 mmHg within one minute5. The position is also recommended by the American College of Gastroenterology for managing nighttime GERD symptoms, since the entire-body angle prevents acid reflux more effectively than just bending at the waist.
When it’s used at home:
– Post-neurosurgery recovery (physician-directed ICP management)
– Severe GERD that doesn’t respond to Semi-Fowler’s alone
– Some bariatric patients who find Fowler’s positions uncomfortable
Modified Trendelenburg / Passive Leg Raise
Full Trendelenburg tips the entire body head-down, which raises intracranial pressure and isn’t safe for many home care patients. Modified Trendelenburg solves this: the patient lies flat on their back at 0 degrees while only the leg section of the bed elevates.
This is the modern, safer alternative for two common home care needs:
- Severe leg and foot swelling (edema) — Isolated leg elevation promotes venous return without the risks of a full head-down tilt. For patients with chronic venous insufficiency or post-surgical swelling, this is the standard intervention.
- Hemodynamic support — A passive leg raise (lifting the legs to roughly 45 degrees while the torso stays flat) is used as a quick, reversible test of fluid responsiveness and a temporary measure for low blood pressure episodes.
Unlike Zero Gravity, which distributes weight evenly across the whole body, Modified Trendelenburg focuses specifically on draining fluid from the lower extremities. Any full-electric hospital bed with independent leg-section control can achieve this position.
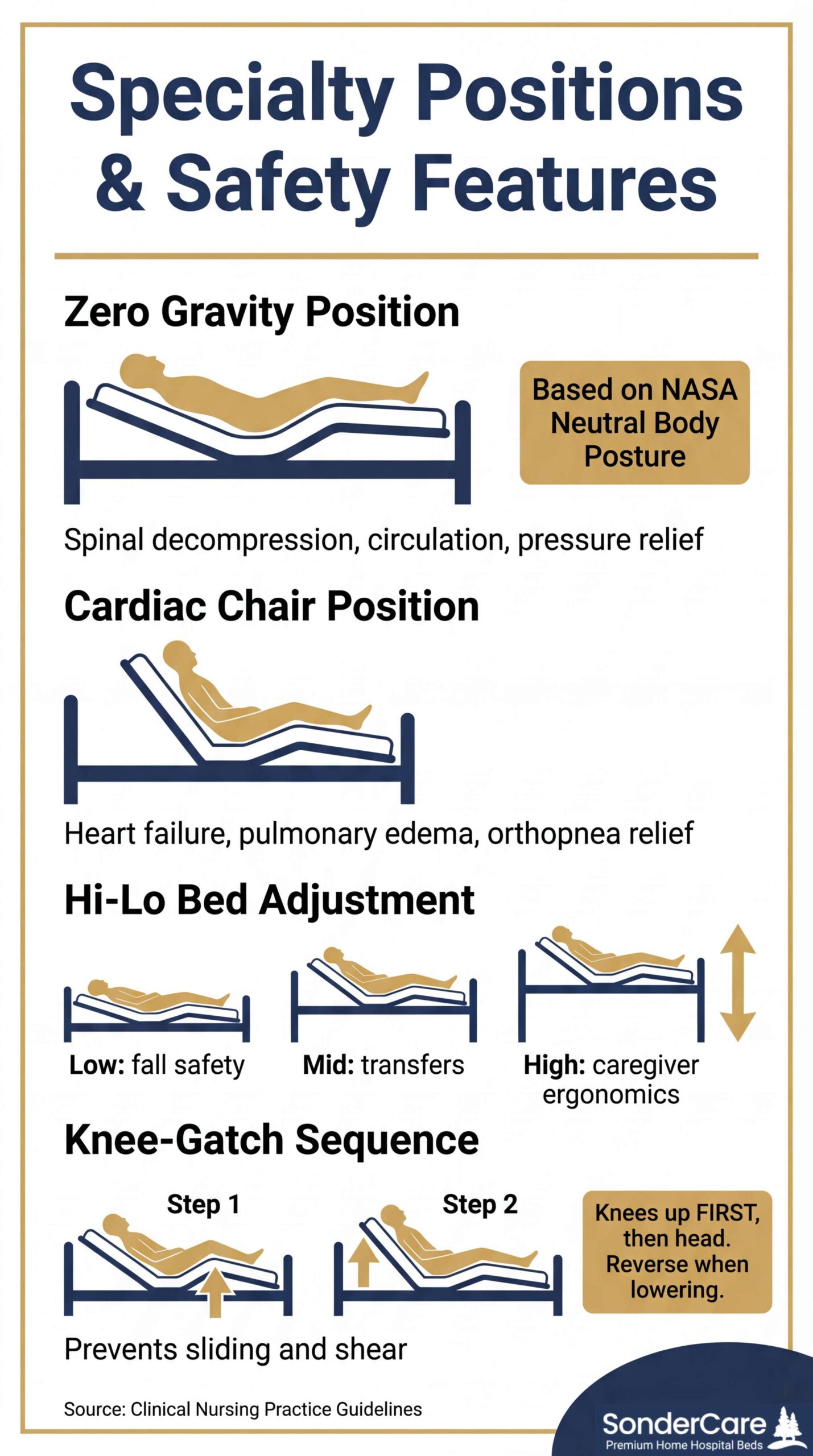
Zero Gravity Position
The zero gravity position comes from NASA’s Neutral Body Posture research — the shape the human body naturally assumes when no gravitational force acts on it. NASA developed this posture to protect astronauts’ spines during launch and re-entry. The adjustable bed and hospital bed industries have since adopted it as a comfort and therapeutic standard.
In zero gravity, the body reclines with approximately 128 degrees between the torso and knees, and about 133 degrees between the upper and lower legs. Both the head and knees are slightly elevated, with the legs roughly parallel to the abdomen. The heart sits below both the raised upper body and the elevated legs, creating even weight distribution and a sensation of weightlessness. Think of it as an Adirondack chair taken further — the legs elevate above heart level and body weight spreads across the entire surface rather than concentrating at the hips and shoulders.
How Hospital Beds Achieve Zero Gravity Differently
Consumer adjustable beds create zero gravity through articulation alone — raising the head and foot sections independently. It works, but it’s limited.
Hospital beds like the SonderCare Aura Premium achieve a more complete zero gravity by combining three separate movements:
- Backrest elevation — the head section raises to incline the upper body
- Knee break elevation — the knee section raises to bend the legs at the correct angle
- Whole-frame tilt — the entire bed frame tilts as one unit, independent of the articulation above
That third component — the frame tilt — is what separates hospital bed zero gravity from consumer bed zero gravity. A gentle Reverse Trendelenburg tilt (typically 10-15 degrees) adds gravitational redistribution on top of the section adjustments. The articulation creates the body contour. The tilt fine-tunes the gravitational angle across the whole body. Together, they produce the full weightless, cradled sensation.
Therapeutic Benefits of Zero Gravity
- Spinal decompression — Maintains the spine’s natural S-curve and reduces compression on vertebrae, helping relieve back pain
- Improved circulation — Elevating the legs above heart level promotes venous return and reduces leg and foot swelling (edema)
- Reduced pressure points — Even weight distribution lowers the risk of pressure ulcers for patients with limited mobility
- Respiratory support — Slight upper-body elevation opens airways, may reduce snoring and sleep apnea symptoms, and helps manage GERD
- Less shear and sliding — The combination of articulation and frame tilt reduces the sliding forces that occur when only the head section is raised, a common cause of skin breakdown in bed-bound patients
Supine Position (Flat on Back)
The baseline: patient lies flat on their back at 0 degrees. While it sounds simple, supine carries real risks for certain patients.
The Drakulovic randomized trial demonstrated that supine positioning increased nosocomial pneumonia rates to 34% compared to 8% in patients elevated to 45 degrees1. For patients with swallowing difficulties, lying flat significantly increases aspiration risk.
When supine is appropriate:
– Spinal alignment procedures (physician-directed)
– Certain post-surgical recovery protocols
– Brief periods for repositioning and skin checks
When to avoid it:
– Patients with dysphagia (swallowing difficulty)
– Active GERD or reflux
– Congestive heart failure or pulmonary edema
– Anyone at risk for aspiration pneumonia
Even when supine is appropriate, proper support matters. Place pillows under the lumbar area, flex the knees 5-10 degrees, and elevate heels off the mattress to prevent pressure buildup at the occiput, sacrum, and heels.
Prone Position (Face Down)
The patient lies on their stomach. This is the most dramatic position change and requires careful execution with proper head and arm placement.
Prone positioning gained widespread attention during the COVID-19 pandemic for its role in treating severe ARDS. The landmark PROSEVA trial showed that prolonged prone sessions reduced 28-day mortality from 32.8% to 16.0% in patients with severe acute respiratory distress syndrome6.
Home care considerations: Prone positioning at home should only be done under direct medical guidance. It requires careful monitoring of pressure points (forehead, chin, shoulders, chest, knees) and is physically demanding for caregivers. A bed with independent section control makes repositioning safer and less strenuous.
Lateral Position (Side-Lying)
The patient lies on their side. The 30-degree lateral tilt is the most clinically important variation for home care.
30-Degree Lateral Tilt
International pressure injury prevention guidelines from the NPUAP/EPUAP/PPPIA recommend the 30-degree lateral tilt to offload pressure from the sacrum and greater trochanter7. This specific angle redistributes body weight away from the bony prominences where pressure ulcers develop.
For patients at higher BMI, a 40-degree angle may be needed to effectively offload the sacrum.
When to Use Lateral Positioning
- Pressure injury prevention — Alternate between supine and both lateral sides on a regular turning schedule
- Airway drainage — Helps clear secretions in patients with respiratory conditions
- Sleep comfort — Many patients find side-lying more comfortable than supine, especially those with lower back pain
Use pillows or wedges between the knees and behind the back to maintain the position. Beds with specialty pressure redistribution mattresses help reduce interface pressure during lateral positioning.
Sims’ Position (Semi-Prone)
A variation of lateral that home caregivers encounter frequently on discharge papers. The patient lies on their left side, halfway between lateral and prone. The left arm tucks behind the back, the right arm extends forward, the left leg stays mostly straight, and the right knee draws up toward the chest.
Sims’ is the standard nursing position for administering enemas and rectal suppositories — tasks that come up regularly in home care. It’s also effective for airway drainage in patients with reduced consciousness and provides unique pressure relief off the sacrum that differs from a straight lateral tilt. If you see “place patient in Sims’ position” on care instructions, this is what they mean.
Cardiac Chair Position
This position mimics sitting in a recliner: the back is elevated to roughly 60-65 degrees while the legs rest in a slightly bent, lowered position. It’s not a single standardized angle — manufacturers program it differently.
The 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure supports upright positioning as a first-line supportive measure for patients with acute decompensated heart failure and pulmonary edema8. The cardiac chair position:
- Improves diaphragmatic mechanics for easier breathing
- Reduces venous return to decrease fluid overload
- Relieves orthopnea (the feeling of breathlessness when lying flat)
For patients who spend extended time in bed, the cardiac chair preset provides a comfortable seated position without transferring to an actual chair — reducing fall risk during transitions.
Hi-Lo Adjustment: The Position Everyone Overlooks
While not a body position per se, bed height is arguably the most used “position” in daily caregiving. Hi-lo adjustment raises or lowers the entire bed frame.
Low position (closest to the floor): Reduces injury severity if a patient rolls or falls out of bed. The SonderCare Aura Premium drops to an ultra-low position that minimizes the distance to the ground — a critical safety feature for patients with dementia, restlessness, or seizure risk.
Raised position (caregiver working height): Elevating the bed to waist height prevents caregiver back injuries during repositioning, wound care, bathing, and transfers. Ergonomic guidelines recommend caregivers work at elbow height to avoid stooping.
Transfer height: A mid-height that matches wheelchair or commode seat level for safe patient transfers.
The Knee-Gatch: A Safety Step Most Caregivers Skip
Here’s a positioning mistake that causes real harm. When you raise a patient into Fowler’s position, gravity pulls them down toward the foot of the bed. This sliding creates shear — a friction force that tears fragile skin and ranks among the leading causes of pressure injuries in bed-bound patients.
The fix is simple: raise the knee section 10-15 degrees before raising the head. This “knee-gatch” or “knee break” anchors the patient’s hips in a bucket-like seat, stopping the slide before it starts.
Premium home hospital beds like the SonderCare Aura models feature Auto-Contour — the bed automatically raises the knees when the head section goes up. You don’t have to remember the sequence because the bed handles it. If your bed doesn’t have Auto-Contour, make it a habit: knees up first, then head up. Reverse the order when lowering (head down first, then knees).
Which Positions Does Your Home Hospital Bed Actually Support?
Not all beds are created equal. Here’s what to check:
| Position | Consumer Adjustable Bed | Semi-Electric Hospital Bed | Full-Electric Hospital Bed |
|---|---|---|---|
| Fowler’s variations | Head only (limited angle) | Yes | Yes |
| Trendelenburg | No | Manual crank only | Yes (motorized) |
| Reverse Trendelenburg | No | Manual crank only | Yes (motorized) |
| Hi-Lo adjustment | No | Manual crank | Yes (motorized) |
| Cardiac Chair preset | Rarely | No | Select models |
| Zero Gravity (full) | Articulation only | No | Yes (articulation + tilt) |
| Modified Trendelenburg | Foot section only | Manual crank | Yes (motorized) |
| Auto-Contour (knee-gatch) | No | No | Premium models |
| Programmable presets | Basic | No | Premium models |
Consumer adjustable beds (the kind sold at mattress stores) typically adjust only the head and foot sections. They cannot tilt the full frame for Trendelenburg or Reverse Trendelenburg, and they lack hi-lo adjustment entirely. If your care plan requires clinical positioning, you need a full-electric home hospital bed.
The SonderCare Aura line bridges this gap by offering full clinical positioning — Fowler’s, Trendelenburg, Reverse Trendelenburg, cardiac chair, and hi-lo — in a residential-style frame that doesn’t look institutional.
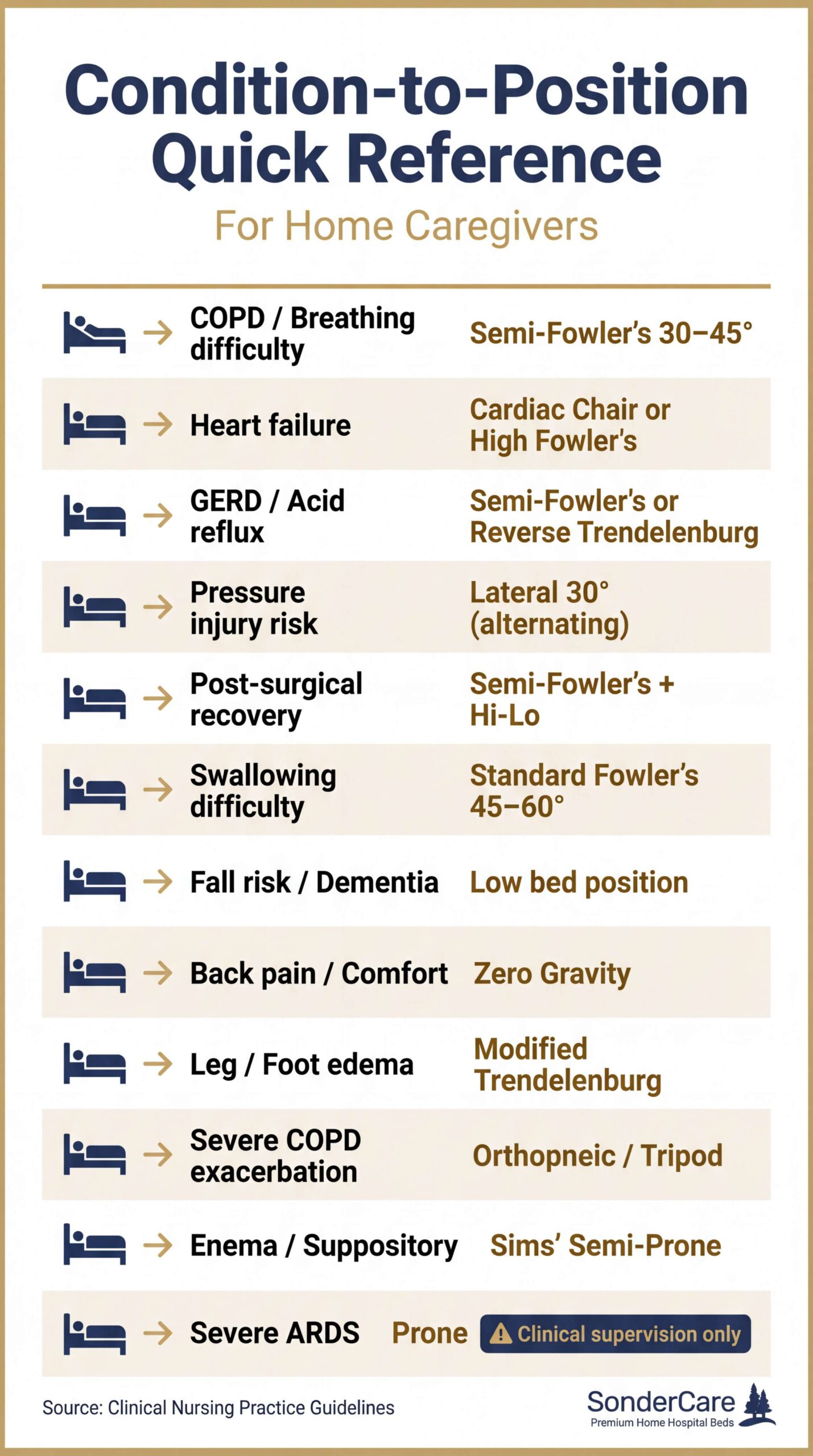
Condition-to-Position Quick Reference
Not sure which position helps with which condition? Use this table:
| Condition | Recommended Position(s) | Why |
|---|---|---|
| COPD / breathing difficulty | Semi-Fowler’s (30-45 degrees) | Opens airway, drops diaphragm |
| Congestive heart failure | Cardiac Chair or High Fowler’s | Reduces venous return, eases dyspnea |
| GERD / acid reflux | Semi-Fowler’s or Reverse Trendelenburg | Gravity prevents acid backflow |
| Pressure injury risk | Lateral 30-degree tilt (alternating) | Offloads sacrum and trochanter |
| Post-surgical recovery | Semi-Fowler’s + hi-lo for transfers | Breathing comfort + safe mobility |
| Swallowing difficulty | Standard Fowler’s (45-60 degrees) | Reduces aspiration risk |
| Fall risk / dementia | Low bed position (hi-lo at minimum) | Minimizes fall injury severity |
| Back pain / general comfort | Zero Gravity | Decompresses spine, promotes circulation |
| Leg/foot edema (swelling) | Modified Trendelenburg | Drains fluid from lower extremities |
| Severe COPD exacerbation | Orthopneic (Tripod) | Maximum diaphragm drop + accessory muscles |
| Enema / rectal suppository | Sims’ (Semi-Prone) | Standard nursing position for administration |
| Severe ARDS | Prone (clinical supervision only) | Improves oxygenation dramatically |
Frequently Asked Questions
What is the most common hospital bed position for sleeping?
Semi-Fowler’s position (30-45 degrees) is the most commonly recommended sleeping position for patients with respiratory or cardiac conditions. For patients without specific medical needs, a slight 15-20 degree elevation (Low Fowler’s) provides comfortable sleep while reducing reflux risk.
Can a regular adjustable bed do Trendelenburg position?
No. Consumer adjustable beds only bend the head and foot sections — they cannot tilt the entire bed frame. True Trendelenburg requires a hospital-grade bed with full-frame tilt capability. This is one of the key differences between a home hospital bed and a consumer adjustable bed.
How often should I reposition a bedridden patient?
Clinical guidelines recommend repositioning every two hours to prevent pressure injuries, alternating between supine, left lateral (30 degrees), and right lateral (30 degrees). However, the optimal schedule depends on the patient’s skin condition, mattress type, and mobility level. A pressure redistribution mattress can extend safe intervals, but never replace repositioning entirely.
What’s the difference between Fowler’s and Reverse Trendelenburg?
In Fowler’s position, the back section of the bed bends upward while the base stays flat — the patient is essentially sitting up in bed. In Reverse Trendelenburg, the entire bed frame tilts as one unit so the head is higher than the feet while the patient remains flat. Fowler’s flexes the body at the hips; Reverse Trendelenburg keeps the body straight.
Which hospital bed position helps with breathing?
Semi-Fowler’s (30-45 degrees) is the standard starting position for respiratory difficulty. For acute distress, High Fowler’s (60-90 degrees) provides maximum lung expansion. The cardiac chair position also helps patients with heart failure breathe more easily by reducing fluid pressure on the lungs.
Getting Clinical Positioning Right at Home
Knowing hospital bed position names isn’t about memorizing medical terminology. It’s about understanding that a 30-degree elevation isn’t the same as 60 degrees — and that the difference could affect your loved one’s breathing, skin integrity, or recovery.
If your care situation requires precise positioning — and most home healthcare situations do — invest in a bed that actually delivers these positions reliably. A full-electric home hospital bed with programmable presets takes the guesswork out of clinical positioning and gives you confidence that “raise to Semi-Fowler’s” means pressing one button, not eyeballing an angle.
Contact SonderCare to discuss which bed positions your care plan requires and which model fits your home.
References
- Drakulovic, M. B., Torres, A., Bauer, T. T., Nicolas, J. M., Nogue, S., & Ferrer, M. (1999). Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. The Lancet, 354(9193), 1851-1858. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(99)04465-1/fulltext
- Logemann, J. A., et al. Videofluoroscopic swallowing study examining the effect of reclined posture on aspiration risk in dysphagic patients. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC8754510/
- Klompas, M., et al. (2022). Strategies to Prevent Ventilator-Associated Pneumonia in Acute Care Hospitals: 2022 Update. Infection Control & Hospital Epidemiology. https://www.cambridge.org/core/journals/infection-control-and-hospital-epidemiology/article/strategies-to-prevent-ventilatorassociated-pneumonia-in-acute-care-hospitals-2022-update/4F75502961624969B5952467A5C40E6A
- Systematic review and meta-analysis of 16 studies on Trendelenburg position hemodynamic effects (2024). Journal of Vascular Anesthesia. https://pubmed.ncbi.nlm.nih.gov/39500675/
- Feldman, Z., et al. Effect of head elevation on intracranial pressure, cerebral perfusion pressure, and cerebral blood flow in head-injured patients. Journal of Neurosurgery. https://pubmed.ncbi.nlm.nih.gov/11773818/
- Guerin, C., Reignier, J., Richard, J. C., et al. (2013). Prone positioning in severe acute respiratory distress syndrome. New England Journal of Medicine, 368(23), 2159-2168. https://www.nejm.org/doi/full/10.1056/NEJMoa1214103
- National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, & Pan Pacific Pressure Injury Alliance. (2014). Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. https://npiap.com/
- Heidenreich, P. A., et al. (2022). 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. Journal of the American College of Cardiology, 79(17), e263-e421. https://www.jacc.org/doi/10.1016/j.jacc.2021.12.012







